
Thoracic Mobility: Important for Every Sport and Movement in Life!
Do you have low back pain, shoulder pain, or neck pain? Do you want to improve your golf swing, overhead serve in volleyball, hitting power in baseball and softball, or pitching velocity?
Do you have low back pain, shoulder pain, or neck pain? Do you want to improve your golf swing, overhead serve in volleyball, hitting power in baseball and softball, or pitching velocity?

As a physical therapist, the thoracic spine is one of first areas I treat. Whenever you lift your arm overhead, throw a ball, swing a golf club, or even look up at a book on a high shelf, your thoracic spine is moving.Try this: relax your upper back and shoulders and get really slouchy in your chair. Now try looking up at the ceiling. Then try lifting your arm overhead… Hard right? Now sit up nice and tall in your chair and perform the same two movements. Should be much easier, more comfortable, and you should be able to get more range of motion in your neck and shoulder. I know this is a very extreme example but imagine how much even a little bit of thoracic spine stiffness can affect how you get your arms overhead to spike a ball in volleyball or throw a baseball.Common problems associated with poor thoracic mobility include shoulder impingement/pain, low back pain, and neck pain. There are other factors that can contribute to these same issues but, in this article, we are going to focus on the thoracic spine as the root of the problem. When the thoracic spine doesn’t move, your low back starts to pick up the slack. Instead of getting normal extension through your thoracic spine you end up hyperextending through your lumbar spine. This repetitive lumbar hyperextension leads to pinching posteriorly of the bones in your low back, thus resulting in pain. The same issues can happen at your neck.
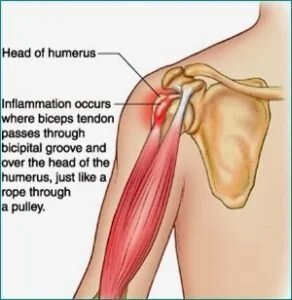
When you lift your arm overhead and you cannot extend in the thoracic spine, what will typically happen is your humerus will jam up against the acromion (See picture below). Having this bone to bone contact overtime can lead to pain. This same issue can also lead to rotator cuff muscle microtears because the rotator cuff muscle sits right underneath the acromion, and the friction of the constant bone to bone contact can lead to fraying of the muscle underneath.
From a performance perspective in overhead athletes or overhead lifting (push press, push jerk, overhead squat), more force can be generated and more weight can be lifted when you have the range of motion to complete the movement. To properly engage your shoulder blade muscles and have your shoulder blade sit properly on the ribcage, you need full range of motion of the shoulder joint and thoracic spine. If not, like we mentioned before, your shoulder blades will sit forward on your ribcage (like with bad slouching posture) and your shoulder blade muscles won’t be able to engage properly. The better your shoulder blade muscle strength and stability are, the more power you can generate and the more weight you can lift overhead.Imagine swinging a baseball bat if you can’t rotate your thoracic spine. With this limitation the force you can produce when you hit the ball will be considerably less as compared to being able to rotate your spine fully.Here are some exercises you can do on your own to address this area of the body:7 Common Reasons Why You Have Shoulder Pain
Shoulder pain is one of my favorite issues to treat. For me, shoulder pain is easy to treat. Why? Because there are a lot of commonalities among individuals that come to me with shoulder pain, no matter what type of shoulder pain it is. No, not everyone with shoulder pain will have the same exact 3 or 4 problems; which is why an extensive examination is necessary before I start treating someone. However, I still find that most of my shoulder pain patients have a few things in common. Listed below are the top 7 dysfunctions I see in my shoulder patients:1. Restricted pectoralis minor/major flexibilityYou will notice difficulty reaching behind your back
2. Restricted latissimus dorsi flexibilityYou will notice difficulty raising your arm to your ear
3. Trigger points (muscle knots) that refer pain into the shoulderIf you apply deep pressure to certain muscles, you will feel tender points that refer pain elsewhere (especially common with the rotator cuff muscles that sit on top of your shoulder blade)
4. Forward head and shoulder postureMost people have sitting jobs and tend to sit with slouchy posture
5. Overactivation of the upper trapezius musclesYou will notice you constantly shrug your shoulders up when lifting your arm overhead
6. Weak scapular retractors, core, and rotator cuff muscles
7. Poor motor controlYou have the range of motion but your body doesn’t engage the right muscles at the right time appropriately to perform a specific movement
Next I want to talk about some common diagnoses I hear when a patient walks into my facility.Pain in the biceps or the front of the shoulder: A lot of times people come in with pain in the front of the shoulder and have been told they have a biceps tendonitis/tendonapathy. If you hear this diagnosis it means your biceps tendon has taken on extra work because your rotator cuff muscles, your scapular stabilizers and your core are slacking on the job. Other common issues found with this diagnosis include: restricted thoracic mobility, and slouchy forward head and shoulder posture, tight pectoralis minor/major muscles, and potentially tight latissimus dorsi muscles.
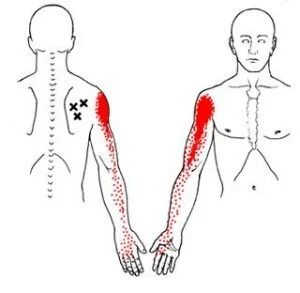
Pain that travels from the top of your shoulder down your arm an inch or two? This sensation is commonly due to what we call active trigger points (inflamed muscle knots). Your rotator cuff muscles, which sit on top of the shoulder blade, can develop trigger points that can refer pain into the shoulder and, at times, down the arm. Performing soft tissue massage using the lacrosse ball on tender or tight spots will help calm down the muscle and reduce the feeling of pain traveling into your shoulder.
Pain at the top of the shoulder joint and pain with raising your arm to end range overhead: This type of pain is typically given the diagnosis of shoulder impingement/ bursitis. This occurs because the humerus (arm bone) basically jams into the top of the shoulder joint whenever you raise your shoulder overhead. These people typically have bad forward head and shoulder posture. This diagnosis is either due to excessive shoulder mobility, or it is due to tight shoulder musculature (pectoralis minor/major, lats, rotator cuff muscles), overuse of the upper trapezius muscles, restricted thoracic mobility, or the inability to use your back, shoulder blade and core muscles efficiently. The latter option I tend to see more often.

Shoulder pain that is associated with weakness and, at times, the inability to lift your arm overhead: This injury can result from a traumatic fall or gradual wear and tear of the muscle with overhead activity. Common issues I see with this diagnosis include: forward head and shoulder posture, restricted thoracic mobility, tight shoulder musculature (pectoralis minor/major, latts, Rotator Cuff muscles), overuse of the upper trapezius muscles, and you are not using your back, shoulder blade and core muscles efficiently.

Notice a trend with some of the different diagnoses?.. It may seem like I am repeating myself a lot but most shoulder diagnoses stem from the same problems (excluding traumatic shoulder injuries of course). If you have shoulder pain and are reading this article then attacking the 7 problems I have listed above is a good place to start.Patellar Tendinopathy (Jumpers Knee):
Have you ever had pain in the front of the knee with jumping, cutting, running, or kicking? I personally have and it stinks. I played soccer growing up so the feeling of a sharp jolt to the front of the knee is not something foreign to me. To those of you experiencing the same sharp pain to the front of the knee, you will know that it feels as if you are running or jumping on eggshells.
What Is It and How Do You Treat It?
Have you ever had pain in the front of the knee with jumping, cutting, running, or kicking? I personally have and it stinks. I played soccer growing up so the feeling of a sharp jolt to the front of the knee is not something foreign to me. To those of you experiencing the same sharp pain to the front of the knee, you will know that it feels as if you are running or jumping on eggshells. You want to be explosive but you feel like if you bend your knees too much to really generate power or to absorb a landing, the sharp jolt is just waiting for you not far behind. I experienced this pain as a soccer player but it affects many other sports such as basketball, volleyball, tennis, track and field, football and the recreational runner. Athletes between the ages of 15 to 30 are primarily affected, with men more commonly affected than women. By definition, patellar tendinopathy (Jumper’s knee) is an overuse injury thought to be caused by excessive or repetitive forces applied to the patellar tendon. Signs and Symptoms of Patellar Tendinopathy:
Anterior knee pain over the patella tendonTenderness at the inferior pole of the patellar tendonPain made worse with jumping, landing, cutting/pivoting, or running activitiesPain with stairs, squatting, and at times prolonged sittingOnset of pain is usually gradual and commonly related to an increase in sport activityThe feeling of stiffness in the patellar tendon in the morningIncreased thickness of the patellar tendon compared to the opposite side
What is the Function of the Patellar Tendon?
The patellar tendon attaches directly from the tibial tuberosity to the inferior tip of the patella (knee cap). The quadriceps muscle attaches into the superior tip of the patella, thus transmits forces through the patellar tendon based on the common attachment into the patella. Therefore, any tightness or weakness in the quadriceps pulls on the patellar tendon. The patellar tendon also functions in the storage and release of energy when you jump, run, cut or pivot. This means there is a lot of load that has to transfer through the patellar tendon so overtraining, insufficient rest, faulty movement patterns, mobility impairments, and hip, core and foot weakness can contribute to the development of patellar tendinopathy.
Common Impairments Found in Individuals with Patellar Tendinopathy:
Hip Abductor and Hip External Rotator WeaknessAltered Hip and Knee Movement Patterns upon Landing (Poor Movement Quality)Excessive or Restricted Hip and Ankle MobilityLook for reduced dorsiflexion, quadriceps or hamstring tightness, hip Internal rotation mobility, increased varus foot alignment, etc.
Quadriceps WeaknessExcessive Foot Pronation: foot collapses inward upon landing which causes knee valgus (knee collapse inward) as well as the femur to then internally rotate excessively
Rehabilitation Focus:
Eccentric Quadriceps StrengtheningQuadriceps and Hamstring FlexibilityHip Abduction and External Rotation StrengtheningMovement Competency–May require Cueing from a Rehab Professional or Qualified Strength Coach to address running, cutting, and jumping mechanicsFoot and Ankle StrengtheningAnkle Dorsiflexion Range of Motion
Exercise Ideas:
Here are some exercise ideas to get you started but it is always helpful to seek help from a medical professional.Quadriceps Flexibility:Couch Stretch: https://www.youtube.com/watch?v=tABeNRBDf30
Hip External Rotation Strengthening:Clamshell: https://www.youtube.com/watch?v=2OhR279AWNYFire Hydrant (can add band around knees to increase difficulty): https://www.youtube.com/watch?v=0Vk6BrtikL8Side Plank with Clamshell: https://www.youtube.com/watch?v=82tKGsLrADY
Hip Abduction Strengthening:Sidelying Hip Abduction: https://www.youtube.com/watch?v=Ku6QkDJqdwYSide Plank: https://www.youtube.com/watch?v=TPp92f8HlG0
Ankle Dorsiflexion:Mobilization with Movement: Long Sitting Position with Mobility Band: https://www.youtube.com/watch?v=sBCMIaIkP8cWall Stretch: https://www.youtube.com/watch?v=9QRVlaw9QWM
References:
Malliaras, P., Cook, J., Purdam, C. and Rio, E. (2015). Patellar Tendinopathy: Clinical Diagnosis, Load Management, and Advice for Challenging Case Presentations. Journal of Orthopaedic & Sports Physical Therapy, 45(11), pp.887-898.
Mendonça, Luciana D., et al. “Association of Hip and Foot Factors With Patellar Tendinopathy (Jumper’s Knee) in Athletes.” Journal of Orthopaedic & Sports Physical Therapy, vol. 48, no. 9, 2018, pp. 676–684., doi:10.2519/jospt.2018.7426.
Baseball Specific Screening
The OnBase University screening stems from the belief that there is not only one technically correct way to play baseball or softball. There are an infinite number of ways to play the game. The best baseball players in history don’t all hit or pitch the same way, but they do have some commonalities in their styles that have allowed them to be the best. The aim of a good coach or trainer is to find the one efficient style that works for that player, and that is based on what the player can physically do. If we can match an athlete’s physical ability to his/her technical skills, it will help the player play at his/her highest level possible.Coach and Player Goals: To be Efficient and PowerfulWhat makes a hitting or pitching style Efficient?
It is ReproducibleThe player has command over their pitching/hitting styleThe player is able to maximize his/her power with the least amount of effort
What makes a hitting or pitching style Powerful?
Proper Kinematic Sequencing: how energy is transferred from the ground through the body to the ball or bat
It’s up to the coaches to guide the player into what kind of hitting or pitching style the athlete uses. Our goal is to assist the coach and player by determining how the athlete’s physical abilities relate to their technical skills. Pitching and hitting requires involvement from the whole body, from the feet all the way through to the neck, shoulders, elbow and hand. If there is a breakdown anywhere in this chain, it could lead to poor power, poor contact on the ball for hitters, inconsistency, and pain or injury. How is your body limiting your performance and where exactly are the breakdowns? That’s what we want to find out.How do we determine where the breakdowns are?Through Movement Screening: Functional Movement Screening (FMS), Y balance testing, OnBase University pitching and hitting screening, VALD forceplate testing, dynamometer and joint by joint assessment.We will provide these findings to you, your pitching or hitting coach, and your fitness coach to develop a team approach in order to help you become a better athlete.Let us help you and your coaches. Call us at 407-718-0437 or email us at rachel@jsportsrehab.com..Reference: http://www.onbaseu.com