
Staying Strong on the Court: A Tennis Player's Guide to Injury Prevention in Orlando
Tennis is one of the most demanding sports on the body — full of quick direction changes, repetitive swinging, and explosive movements. Whether you're a weekend player or competing in a local league multiple times a week, the sport puts real stress on your shoulders, elbows, knees, and hips over time. At J Sports Rehabilitation, we work with tennis players of all ages and skill levels across Orlando to help them stay on the court and play at their best.
Why Tennis Players Get Hurt
Orlando's tennis community is competitive, and many recreational and league players log serious court time — some playing several days a week. That kind of volume, combined with the repetitive nature of the sport, creates a perfect setup for overuse injuries. The most common issues we see include:
Tennis elbow (lateral epicondylitis) — from repetitive gripping and the impact of ball contact
Shoulder pain and rotator cuff strain — common with serving and overhead strokes
Knee pain — from the constant lateral movement, pivoting, and stop-start nature of rallies
Lower back strain — often linked to the rotational demands of groundstrokes and serves
Ankle sprains — a result of quick lateral shuffles and sudden direction changes
None of these are limited to any one age group or gender. Younger players pushing hard in competitive matches and older players managing years of accumulated wear and tear both show up in our clinic — the mechanisms are just a little different.
Why Prevention Matters
Most tennis injuries don't come from a single bad moment — they build up over time from repetitive stress, muscle imbalances, or gaps in mobility and strength. The good news is that many of these issues are preventable with the right approach:
Movement screening to catch mobility or stability limitations before they become injuries
Strength and conditioning targeted at the shoulder, core, and lower body to support the demands of the sport
Recovery strategies for players logging frequent court time
Return-to-play plans for players coming back from an injury who want to get back to full intensity safely
At J Sports Rehabilitation, we work one-on-one with players to build a plan around their game, their goals, and how often they're playing — not a generic protocol.
A Note for Orlando's Women's Tennis Leagues
Orlando has a strong and growing women's tennis community, with USTA women's leagues and local club play drawing players of all ages and NTRP levels throughout the year. We see a lot of women in these leagues dealing with the same overuse patterns — shoulder fatigue from serving, elbow pain from repetitive strokes, and knee or hip discomfort from the demands of doubles and singles play across a long season.
If you're playing in a women's league here in Orlando, a few things are worth knowing:
League play adds up. Multiple matches a week during a season means less recovery time between sessions, which can accelerate overuse injuries if your body isn't prepared for the volume.
Doubles and singles stress the body differently. Singles demands more court coverage and conditioning; doubles often means more reactive, quick-twitch movements at the net. Your training should reflect which one you play most.
A quick check-in can catch small issues early. Many players wait until pain is affecting their game to seek help. Addressing tightness, weakness, or asymmetry before your season ramps up can keep you playing through the whole schedule instead of sidelined mid-season.
Whether you're gearing up for league play, working through nagging pain, or just want a tune-up before the season heats up, we'd love to help you stay competitive and injury-free.
Ready to Play Pain-Free?
If you're dealing with tennis-related pain, or want a proactive plan to keep playing at your best, our team specializes in working with athletes just like you. Schedule an evaluation at our Baldwin Park or Winter Springs location today!
Low Back Pain in Athletes and Adults: How Common It Is, and What Actually Helps
If you're dealing with low back pain right now, you're far from alone. It's one of the most common reasons people come to J Sports Rehab, whether they're a competitive athlete, a weekend warrior, or someone who just spends too many hours at a desk. Here's what the numbers say, and more importantly, what actually helps.
How Common Is Low Back Pain, Really?
According to the CDC's National Health Interview Survey, roughly 39% of U.S. adults reported experiencing back pain within the past three months. That number climbs with age — adults 45 and older report back pain at nearly double the rate of adults in their 20s. Beyond the general population, back pain is also one of the leading causes of missed workdays and the most frequent driver of job-related disability in the country.
Athletes aren't spared either. Repetitive loading from running, throwing, swinging, and jumping puts consistent stress on the lumbar spine, and a huge percentage of sports-related time-loss injuries trace back to the low back or the hips and core stability surrounding it.
The takeaway: if your back hurts, it doesn't mean something is uniquely wrong with you — it means you're dealing with one of the most widespread musculoskeletal issues in the country, and there are proven ways to treat it.
What Actually Helps: Our Approach at J Sports Rehab
1. A Thorough Movement Screen
Before any hands-on treatment or exercise plan, we start with a thorough movement screen. This isn't a quick five-minute look — we assess how you move through your hips, spine, and core, where your strength and mobility limitations are, and what specific patterns might be driving your pain. For athletes, this often includes sport-specific movements (like a golf swing or a throwing motion) to see exactly where the breakdown happens under load.
This step matters because low back pain rarely has one single cause. Two people with the same complaint of low back pain can have completely different underlying reasons for it — one might be missing hip rotation, another might have a core stability deficit, another might simply be compensating for an old ankle injury. A movement screen is what lets us treat the actual cause instead of guessing.
2. Manual Therapy
Low back pain is often tied to tight, overactive muscles, restricted joints, and soft tissue that hasn't been able to heal properly — particularly around the lumbar paraspinals, glutes, and hip flexors. We use a combination of hands-on techniques to address this from multiple angles:
Dry needling targets tight, overactive trigger points directly, helping release tension, improve blood flow, and reduce pain quickly, especially for stubborn tightness that hasn't responded to stretching alone.
Shockwave therapy uses focused acoustic wave pulses to stimulate blood flow and healing in areas of chronic tension or soft tissue irritation, helping jumpstart the body's natural repair process where other treatments have plateaued.
Cupping helps decompress tight fascia and soft tissue, improving local circulation and reducing the sense of tightness that often comes with chronic low back pain.
Soft tissue massage works through superficial and deeper muscle tension, helping calm down irritated tissue and improve mobility before you move into strengthening work.
Joint mobilizations restore normal motion to stiff or restricted segments of the spine and hips, which often contributes to compensation patterns that overload the low back.
Stretching addresses the specific mobility restrictions — often in the hips, hamstrings, or thoracic spine — that force the low back to move more than it should.
We don't use every technique on every patient. Your evaluation determines which combination makes sense for your specific pain and movement limitations.
3. Targeted Exercise
Manual therapy can calm things down, but exercise is what actually fixes the underlying problem. Most low back pain isn't caused by a single injury — it's caused by a movement pattern, a strength deficit, or a mobility restriction somewhere in the kinetic chain (often the hips or core) that puts extra load on the spine over time. A one-on-one physical therapy plan builds strength and control in exactly the areas that are letting you down, so the pain doesn't just come back in a few months.
Why We Combine Manual Therapy and Exercise
At J Sports Rehab, we don't treat low back pain with a single tool. We use manual therapy to calm the tissue and reduce pain in the short term, while building a personalized exercise program that addresses why the pain started in the first place. Every session is one-on-one with the same physical therapist, so your plan evolves as you get stronger, not a generic protocol handed to every patient.
Don't Wait for It to Become Chronic
The longer low back pain sticks around, the more likely it is to become a long-term problem. If you're dealing with back pain that isn't improving on its own, contact us today to schedule an evaluation in Orlando or Winter Springs!
Golf Injuries and TPI Screening: How to Swing Pain-Free

Golf doesn't look like a high-impact sport from the outside, but ask any golfer with a bad back, sore elbow, or aching hip and they'll tell you a different story. The golf swing puts repetitive, asymmetrical stress on your spine, hips, and shoulders — and over time, that adds up. At J Sports Rehab, we work with golfers across Orlando, Winter Park, and Winter Springs who are dealing with exactly this kind of pain, and one of our most valuable tools for helping them is TPI screening.
What Is TPI Screening?
TPI stands for Titleist Performance Institute, and it's the gold standard in golf-specific movement assessment. A TPI screening looks at how your body moves — your hip rotation, shoulder mobility, posture, balance, and core stability — and identifies which physical limitations might be affecting your swing or putting you at risk for injury.
The key idea behind TPI is simple: your swing is a reflection of what your body can and can't do. If you're missing hip rotation, your low back often compensates, which is a common source of golf-related back pain. If your shoulders are tight, your swing mechanics shift in ways that can overload your elbow or wrist. A TPI screening helps pinpoint exactly where those limitations are coming from.
Common Golf Injuries We Treat
Low back pain and stiffness, often the most common complaint among golfers
Golfer's elbow (medial epicondylitis)
Shoulder pain and impingement
Hip tightness or pain, especially on the lead side
Wrist pain from repetitive impact
How TPI Screening Fits Into Your Treatment
A TPI screening isn't just for elite or competitive golfers. Weekend golfers and older adults who want to keep playing pain-free benefit just as much, since it identifies the specific mobility or stability gaps causing the problem, rather than just treating the symptom.
Once we know what's limiting your swing or causing your pain, we build a one-on-one physical therapy plan around it. That might mean improving hip rotation, building rotational core stability, or restoring shoulder mobility, depending on what your screening shows. Because every session at J Sports Rehab is one-on-one with our physical therapists, your plan stays tailored to your body and your swing as you progress.
Ready to Fix the Root Cause?
If golf-related pain has been holding back your game, or you simply want to move better on the course, a TPI screening is a great place to start. Contact J Sports Rehab to schedule your evaluation in Orlando or Winter Springs.
Dry Needling: What It Is and Why It Works

If you've been dealing with a tight muscle, a nagging ache, or pain that just won't loosen up no matter how much you stretch or foam roll, you may have heard other athletes or active adults mention dry needling. It's one of the tools we use most often at J Sports Rehab, and for a lot of our patients in Orlando, Winter Park, and Winter Springs, it's the piece that finally gets them unstuck.
What Is Dry Needling?
Dry needling uses a thin, sterile filament needle inserted directly into a tight band of muscle, often called a trigger point. Unlike acupuncture, which is rooted in traditional Chinese medicine and works with energy pathways, dry needling is a Western medical technique grounded in a musculoskeletal evaluation. The goal is simple: release the muscle tension that's contributing to your pain, restore normal blood flow to the area, and reset how the muscle is firing.
For athletes, this often means faster relief from the kind of deep, stubborn tightness that shows up in the shoulders, hips, calves, or low back after repetitive movement — throwing, running, swinging a golf club, or just sitting at a desk five days a week.
Who Is a Good Candidate?
We use dry needling with a wide range of patients, not just competitive athletes. It's often a great fit if you're dealing with:
Muscle tightness or spasm that hasn't responded to stretching or rest
Chronic pain in the neck, shoulders, low back, or hips
Tendon pain, like golfer's or tennis elbow
Post-injury stiffness that's slowing down your return to sport
Active adults managing everyday aches from work, workouts, or old injuries
What Does a Session Feel Like?
Most patients feel a quick, deep ache or a muscle twitch when the needle reaches the trigger point, followed by a noticeable release in tension. Some soreness afterward, similar to a tough workout, is normal and usually fades within a day or two. It's not the same sensation as a typical injection, and most people are surprised at how manageable it is.
Why We Pair It With One-on-One Physical Therapy
Dry needling on its own can bring short-term relief, but the real value comes from pairing it with a full physical therapy plan. At J Sports Rehab, every session is one-on-one with the same physical therapist, so we can use dry needling as part of a bigger picture — addressing the movement pattern, weakness, or overload that caused the tightness in the first place, not just the symptom.
Our team includes providers trained in Functional Dry Needling (Level 1 and 2), so this isn't an occasional add-on for us; it's a core part of how we treat sports injuries and chronic pain for athletes and active adults across Orlando, Winter Park, Winter Springs, Maitland, and Baldwin Park.
Ready to Get Out of Pain?
If you've been stuck with tightness or pain that isn't improving on its own, dry needling paired with a personalized treatment plan might be exactly what you need. Contact J Sports Rehab to schedule an evaluation and find out if dry needling is right for you.
Meniscus Tears: Why a 17-Year-Old Athlete and a 58-Year-Old Weekend Warrior Shouldn't Be Treated the Same
If you've ever been told you have a torn meniscus, your first question is probably:"Do I need surgery?"
The answer isn't as simple as yes or no.Today's orthopedic surgeons treat meniscus injuries much differently than they did 15 years ago. Rather than removing damaged tissue, the goal is now to preserve as much of the meniscus as possible whenever feasible.The best treatment depends on your age, activity level, type of tear, symptoms, and overall knee health.What Is the Meniscus?
Each knee contains two menisci—crescent-shaped pieces of fibrocartilage that act as shock absorbers between the femur and tibia.The meniscus helps:Distribute force across the kneeImprove joint stabilityProtect the articular cartilageReduce stress that can lead to arthritis
Losing part of the meniscus increases contact pressure within the knee, which is why preserving it has become such an important goal.How Common Are Meniscus Tears?
Meniscus injuries are among the most common knee injuries seen in orthopedics.Research estimates that meniscal injuries requiring operative management occur in approximately 60-70 people per 100,000 each year, and they make up a significant percentage of sports-related knee injuries.In young athletic populations, certain sports carry a particularly high risk because they involve cutting, pivoting, and rapid changes in direction.Common high-risk sports include:SoccerBasketballFootballWrestlingRugbyTennis
One study of young athletes found the greatest rates of isolated meniscus injuries occurred in football (19%), wrestling (13%), and rugby (9%).Young Athletes: Usually an Acute Injury
In teenagers and young adults, meniscus tears often occur after:Twisting on a planted footSudden changes in directionLanding awkwardly from a jumpContact injuries
These athletes frequently remember the exact play when the injury occurred.Because younger patients typically have healthier tissue and better blood supply near the outer portion of the meniscus, surgeons often try to repair the tear rather than remove it.Which Tears Can Be Repaired?
The best candidates for repair include:Vertical longitudinal tearsBucket-handle tearsTears in the outer "red-red" or "red-white" vascular zonesRoot tears in appropriate patientsAcute traumatic tears
Modern surgical techniques have expanded the number of tears that are considered repairable compared with just a decade ago.Although recovery after repair is longer—often 4 to 6 months or more before returning to sport—the long-term goal is preserving knee health.Older Adults: A Different Type of Meniscus Tear
Adults over 40 often develop a different problem.Rather than one traumatic event, the meniscus gradually weakens over time. These are called degenerative meniscus tears.Many people don't remember a specific injury.Instead they notice:Pain with squattingStiffnessSwelling after activityDifficulty kneelingOccasional catching
It's also important to know that many adults have meniscus tears visible on MRI without any symptoms at all.Finding a tear on imaging doesn't automatically mean it is the source of knee pain.Do Degenerative Meniscus Tears Need Surgery?
Not usually.Over the last decade, multiple high-quality studies have shown that many degenerative meniscus tears respond just as well to structured physical therapy as arthroscopic partial meniscectomy, particularly when there is no true mechanical locking of the knee.Physical therapy focuses on:Restoring quadriceps strengthImproving hip strengthNormalizing movement mechanicsImproving balanceReducing joint overload
Surgery may still be appropriate if patients have:Persistent lockingLarge unstable tearsFailure of conservative treatmentCertain root tearsAssociated ligament injuries
Can a Meniscus Tear Heal Without Surgery?
One of the most common questions patients ask is whether a meniscus tear can heal on its own. The answer depends on where the tear is located and what type of tear it is.The outer one-third of the meniscus, known as the "red-red zone," has a relatively good blood supply. Because blood flow is essential for healing, tears in this region—especially in younger individuals—have a greater chance of healing, either on their own or after surgical repair.In contrast, the inner portion of the meniscus, called the "white-white zone," has very little blood supply. Tears in this area are much less likely to heal biologically.However, it's important to remember that not every meniscus tear needs to heal for symptoms to improve. Many people experience significant pain relief and return to their normal activities through physical therapy, strength training, and activity modification, even if the tear remains visible on an MRI.The decision to pursue surgery is based less on the MRI itself and more on factors such as persistent pain, mechanical locking or catching, knee instability, activity goals, and response to conservative treatment.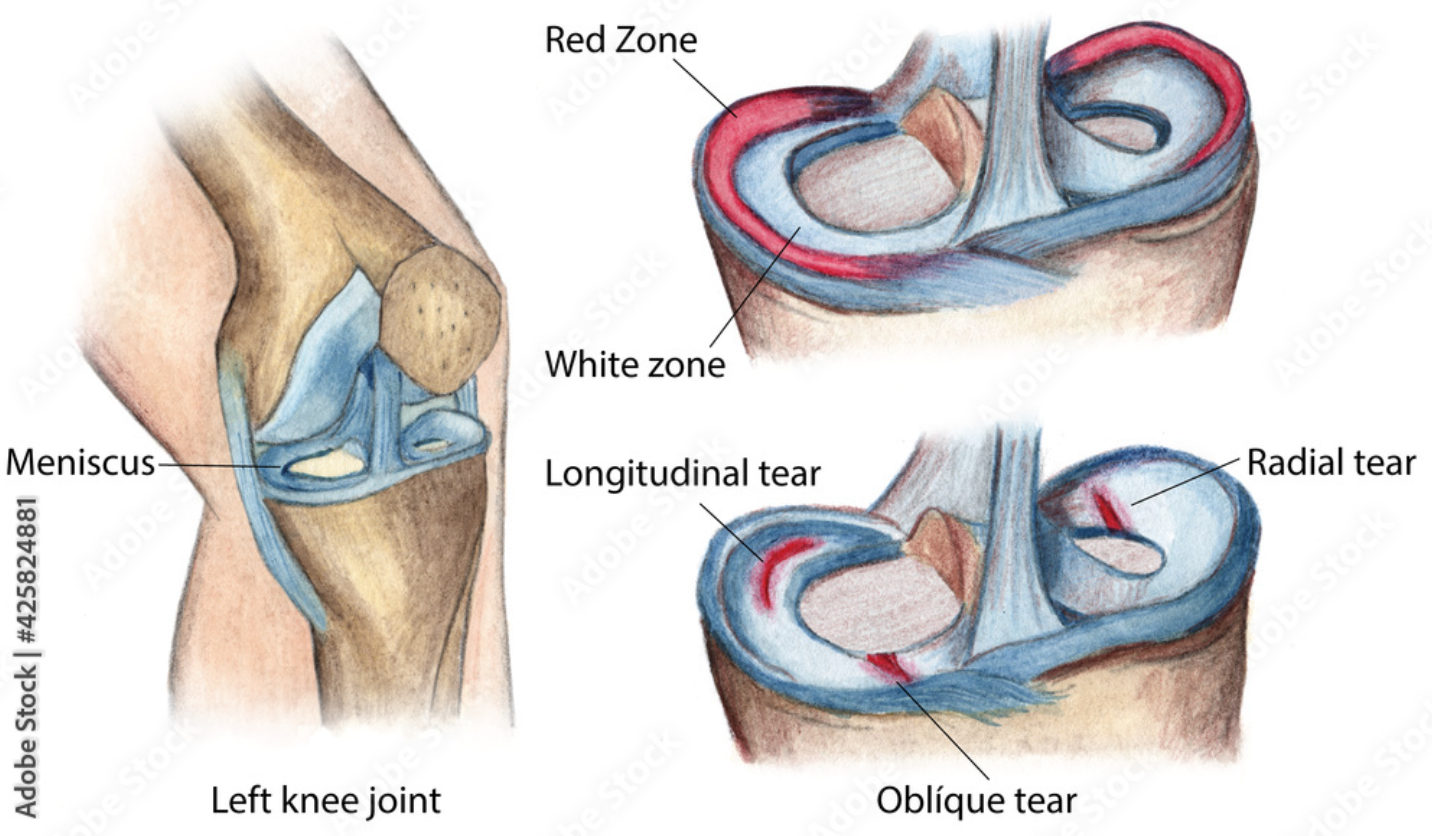
Why Surgeons Remove Less Meniscus Than They Used To
Years ago, surgeons commonly removed torn portions of the meniscus.Today, we know that removing meniscal tissue increases stress on the knee joint and may accelerate cartilage wear over time.Because of this, orthopedic surgeons now follow a simple principle:Preserve the meniscus whenever possible.Even tears that were once considered "irreparable" may now be repaired using newer surgical techniques.What About PRP and Other Biologic Injections?
Patients often ask whether injections can heal a meniscus tear.The answer is: possibly—but the evidence is still evolving.Current biologic treatments being studied include:Platelet-Rich Plasma (PRP)Bone Marrow Aspirate Concentrate (BMAC)
Researchers are investigating whether these treatments may improve healing when combined with meniscus repair or other minimally invasive procedures.While early results are encouraging for selected patients, there is not yet strong evidence that injections alone reliably heal most meniscus tears, and they are generally considered an adjunct rather than a replacement for appropriate rehabilitation or surgery when indicated.Physical Therapy Remains a Cornerstone of Recovery
Whether treatment is surgical or non-surgical, rehabilitation is essential.Physical therapy helps restore:Knee motionStrengthNeuromuscular controlBalanceRunning mechanicsSport-specific movement
For athletes, rehabilitation also includes progressive return-to-sport testing to reduce the risk of re-injury.The Bottom Line
Not all meniscus tears are created equal.A young athlete with an acute traumatic tear may benefit from preserving the meniscus through surgical repair.An older adult with a degenerative tear often improves with physical therapy and activity modification, avoiding surgery altogether.The key is matching the treatment to the individual—not just the MRI.If you're experiencing knee pain, a thorough evaluation can help determine whether your meniscus is truly the source of your symptoms and which treatment option is most appropriateAt our facility, we evaluate athletes and active adults with knee pain to determine whether physical therapy, surgical consultation, or continued activity is the best next step.For The Baldwin Park Location: Call 321-218-0435For The Winter Springs Location: Email Rachel@jsportsrehab.comUnderstanding Little League Shoulder and Little League Elbow

Baseball is one of the most popular youth sports, but the repetitive stress of throwing can place significant demands on a growing athlete's body. Two of the most common overuse injuries seen in young baseball players are Little League Shoulder and Little League Elbow.Who Gets These Injuries?
Little League Shoulder and Elbow most commonly affect baseball players between the ages of 8 and 16, particularly pitchers and athletes who play multiple positions requiring frequent throwing. Because growth plates are still open during these years, young athletes are more susceptible to stress-related injuries than adult players.What Causes Them?
Both conditions develop from repetitive throwing stress over time.Little League Shoulder involves irritation of the growth plate in the upper arm bone (humerus) near the shoulder.Little League Elbow involves stress to the growth plate and soft tissues on the inside of the elbow.Common contributing factors include:Excessive pitch countsPlaying on multiple teams simultaneouslyThrowing year-round without adequate restPoor throwing mechanicsWeakness or mobility deficits in the shoulder, core, hips, and lower bodyReturning to throwing too quickly after soreness or injury
How Can These Injuries Be Prevented?
Follow Pitch Count Guidelines
One of the most effective ways to reduce injury risk is adhering to age-appropriate pitch count recommendations and required rest days. Monitoring total throwing volume—not just pitches during games—is critical.Focus on Proper Mechanics
Efficient throwing mechanics help distribute forces throughout the body instead of concentrating stress on the shoulder and elbow. A qualified pitching coach and movement assessment can help identify mechanical flaws that may increase injury risk.Build Strength Throughout the Entire Body
Throwing is a full-body movement. Athletes should focus on developing:Rotator cuff and scapular strengthCore stabilityHip and glute strengthLower body power and control
A well-designed strength and conditioning program can improve performance while reducing stress on the arm.Listen to Pain
Young athletes should never be encouraged to "throw through" shoulder or elbow pain. Early intervention often prevents minor irritation from becoming a more significant injury requiring extended time away from the sport.When Should You Seek Evaluation?
If a baseball player experiences persistent shoulder or elbow pain, loss of velocity, decreased accuracy, or pain during or after throwing, an evaluation by a sports physical therapist or sports medicine professional is recommended.At J Sports Rehabilitation, we assess mobility, strength, throwing mechanics, and workload management to help athletes recover safely and return to the field stronger than before.Should You Play Through Pain?
When Athletes Should Stop — and When It’s Safe to Continue
Whether it’s during a workout, game, or training session, pain shows up — and most people aren’t sure if it’s something to push through or something to take seriously.I personally have pushed through knee pain and pain from an ankle sprain because I didn’t want to miss out of soccer. I definitely should have stopped playing when I sustained the ankle sprain but, like a lot of athletes, I had my athletic trainer tape me up and I went right back on the field.It's a complicated question but the truth is: not all pain means you have to stop — but not all pain is safe to ignore either.Knowing the difference can be the key to staying active long-term instead of dealing with recurring injuries.Not All Pain Is the Same
Pain is often misunderstood. Many people assume:Pain = damage
But that’s not always the case.Some pain is simply your body adapting to stress, while other types are warning signs that something isn’t functioning properly. The challenge is learning how to tell the difference.When It’s Usually Safe to Continue Activity
There are situations where it’s okay to keep moving — even if you feel some discomfort.✔️ Mild soreness or stiffness: This is common after workouts or new activities. It often improves as you warm up and move more.✔️ Pain that decreases during activity: If your symptoms improve as your body gets moving, it’s often a sign that your tissues are tolerating the load.✔️ Low-level discomfort (not sharp or worsening): A general guideline is that discomfort that stays mild and controlled — and doesn’t get worse during or after activity — is often manageable.When You Should Stop and Get It Checked
On the flip side, some types of pain are not meant to be pushed through.❌ Sharp or sudden pain: This can indicate tissue irritation or injury and should not be ignored.❌ Pain that worsens during activity: If symptoms progressively increase the more you move, your body is likely struggling to handle the load.❌ Swelling or instability: Ankle giving out, knee swelling, or joint instability are strong indicators that something more serious is going on.❌ Pain that lingers or worsens after activity: If you feel worse later that day or the next morning, your body may not be recovering properly.❌ Recurrent pain in the same area: If the same issue keeps coming back, it’s a sign the root cause hasn’t been addressed.What Happens When You Ignore the Warning Signs
Playing through the wrong type of pain can lead to:Repeated injuriesChronic tightness or stiffnessCompensations in other areas (knee, hip, back)Longer recovery timelinesDecreased performance
What starts as a minor issue can turn into something much more difficult to resolve.Why Athletes Often Get This Wrong
Athletes are wired to push through discomfort. That mindset is valuable — but it can also backfire.Common reasons people ignore pain:Fear of missing timePressure from competition or teammatesBelief that rest alone will fix itNot understanding the difference between soreness and injury
The result is often a cycle of temporary relief → return to activity → pain returns.How to Know for Sure
The most reliable way to determine whether it’s safe to continue is through a proper assessment.A sports-focused physical therapist will look at:Movement patternsStrength and controlJoint mobilityLoad toleranceSport-specific demands
This helps determine whether your pain is something you can safely train through — or something that needs to be addressed before it worsens.The Goal Isn’t to Stop — It’s to Stay Active
Good rehab doesn’t mean shutting everything down.In many cases, you can continue training or playing — but with modifications, guidance, and a plan that reduces risk and improves long-term outcomes.The goal is simple: Keep you active now while preventing bigger problems laterFinal Thoughts
Pain during activity doesn’t automatically mean you have to stop — but it also shouldn’t be ignored.Understanding when to push through and when to pull back can be the difference between:Staying consistentOr dealing with recurring injuries and setbacks
If You’re Not Sure What Your Pain Means
If you’re dealing with pain during sport, workouts, or daily activity and aren’t sure whether it’s safe to continue, working with a physical therapist can help you make the right call.At JSR, we help athletes and active adults in Orlando, Winter Park, Baldwin Park, Maitland, and Winter Springs stay active, recover properly, and return to performance with confidence.Why Ankle Dorsiflexion Matters for Performance and Injury Prevention
Ankle dorsiflexion — the ability to bring your foot toward your shin — is one of the most important and commonly overlooked components of athletic movement.Whether you sprint, cut, jump, lift, or change direction, adequate dorsiflexion allows your body to absorb force, maintain alignment, and generate power efficiently. When this motion is limited, the body often compensates up the kinetic chain, increasing stress on the knees, hips, and low back.Why It Matters in Sport
Across all sports, dorsiflexion plays a key role in:Deceleration and change of directionLanding mechanicsSprint mechanicsSquatting and lower body strength trainingForce absorption during contact or cutting
In sports like football, soccer, basketball, and baseball, athletes constantly move in loaded, forward-leaning positions. Limited dorsiflexion can cause early heel rise, knee collapse, or excessive foot rotation — all of which alter mechanics and may increase injury risk.How Much Is Enough?
In weight-bearing testing, we typically look for approximately 40° of ankle dorsiflexion. This range allows athletes to:Stay lower and more stable during cuttingMaintain proper knee alignmentTransfer force efficiently from the ground upwardReduce compensatory stress on surrounding joints
The Bottom Line
If you’re an athlete in Orlando, Winter Park, Baldwin Park, Maitland, or Winter Springs dealing with ankle stiffness, limited dorsiflexion, or recurring knee and Achilles pain, a comprehensive movement assessment can identify whether ankle mobility is limiting your performance.
At JSR in Winter Park, we specialize in sports physical therapy for football players, baseball athletes, runners, and active adults throughout the Orlando area. Our performance-based approach focuses on restoring ankle mobility, improving movement mechanics, and building resilience for return to sport.
If you’re searching for a sports physical therapist near Orlando who understands athlete-specific demands, evaluating and improving ankle dorsiflexion may be the first step toward moving better and performing at a higher level.Below is video showing how we measure the ankle in our facility:Low Back Pain and The Contribution of Hip Flexor Weakness
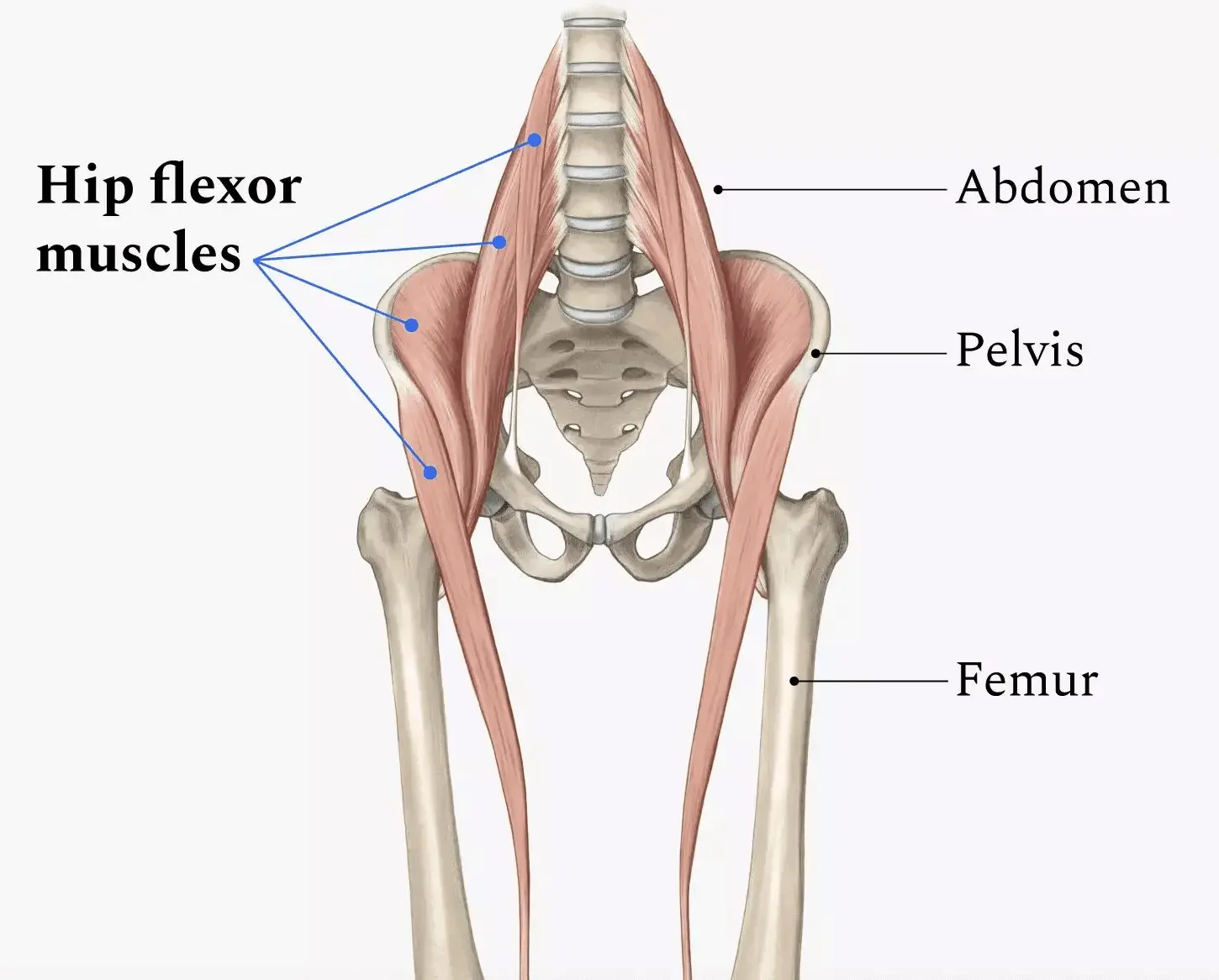
Low back pain is often blamed on the spine itself—but in many active adults, the real driver sits just below it: the hip flexors.The hip flexors (primarily the iliopsoas group) play a major role in controlling pelvic position, stabilizing the spine during movement, and efficiently transferring force between the upper and lower body. When these muscles are weak—not just “tight”—the low back is often forced to compensate.The Hip Flexors’ Role in Spine Support
Hip flexors don’t just lift your leg. They help:Maintain proper pelvic alignmentAssist with trunk stability during walking, running, and liftingControl excessive lumbar extensionWhen they’re strong and functioning well, they reduce unnecessary stress on the lumbar spine
What Happens When Hip Flexors Are Weak
Hip flexor weakness can lead to:Increased lumbar overuse: The low back muscles work harder to stabilize and move the bodyAltered movement patterns: The spine substitutes for hip motion during activities like running, squatting, or getting up from a chairPoor load distribution: Forces that should be absorbed by the hips shift to the lumbar spine
Over time, this compensation can contribute to stiffness, muscle guarding, flare-ups, or persistent low back pain.Why Stretching Alone Often Falls Short
Many people focus on stretching hip flexors when back pain shows up. While mobility matters, stretching without addressing strength can actually worsen instability. A muscle can feel “tight” because it’s weak and overworked—not because it needs more length.The Fix: Strength With Intent
Improving hip flexor strength—especially through controlled, functional movements—helps:Restore proper pelvic controlReduce excess lumbar motionImprove efficiency during sport and daily activity
When the hips do their job, the low back doesn’t have to.Bottom Line
Low back pain isn’t always a back problem. Weak hip flexors can quietly drive compensation, overload, and recurring symptoms. Addressing strength—not just flexibility—can be a key step toward lasting relief and better movement.If back pain keeps coming back despite stretching and rest, it may be time to look at how your hips are contributing.Looking for Lasting Relief From Low Back Pain?
Low back pain is one of the most common reasons people seek physical therapy, especially among active adults, athletes, and individuals with recurring flare-ups. If you’ve tried rest, stretching, or general exercises without lasting results, the issue may not be your spine alone. At JSR we evaluate the entire movement system—especially the hips—to identify strength deficits and movement patterns that contribute to ongoing low back pain. A targeted, individualized approach can help reduce pain, restore function, and keep symptoms from coming back.Below are Exercises that Target the Hip Flexors. They are ordered from easiest to the most difficult. Start with the easiest exercises and work towards the harder ones but take your time with it. It could take months before you work towards the pikes.Start with 2-3 sets of anywhere from 6-20Make sure to always prioritize form over repsDry Needling: How It Helps Reduce Pain and Speeds Up Healing

If you struggle with muscle tightness, nagging pain, or stubborn trigger points that never seem to relax, you may have heard your physical therapist mention dry needling.Dry needling is a proven, research-supported technique used in many sports and orthopedic physical therapy clinics to help decrease pain, improve mobility, and speed up recovery — especially when traditional stretching and massage alone aren’t enough.At JSR, we use dry needling as part of a comprehensive, one-on-one treatment approach to help active adults and athletes move better and feel better — safely.What Is Dry Needling?
Dry needling involves inserting a very thin, sterile filament needle into tight or irritated muscles (often called trigger points).These trigger points can:Cause aching, burning, or sharp painLimit mobilityCreate “tightness” that always comes backRefer pain into other body regions (for example: neck pain creating headaches)
Unlike acupuncture — which is based on Eastern medicine energy pathways — dry needling is rooted in modern musculoskeletal science and focuses on:Resetting irritated nervesReleasing muscle tensionImproving blood flowCalming pain signals in the nervous system
How Does Dry Needling Help Reduce Pain?
When the needle reaches the trigger point, the muscle often produces a small, quick twitch. That twitch response helps “deactivate” the trigger point.Afterward, many people experience:✔ less tightness
✔ improved movement
✔ reduced pain
✔ easier muscle activation during exerciseDry needling can help with conditions such as:Low back painNeck stiffness and headachesShoulder painTennis/golfer’s elbowHip painKnee painChronic tight calves or hamstringsSports injuriesPost-surgical tightness
The key: dry needling isn’t done alone. It works BEST when combined with manual therapy and specific strengthening — so the pain relief actually lasts.Is Dry Needling Safe?
When performed by a licensed and trained physical therapist, dry needling is considered very safe.Most people feel:Potentially mild soreness for 12–24 hoursa sense of muscle “release”Easier movement shortly afterward
Dry Needling and Physical Therapy: Why They Work Well Together
Dry needling can quickly calm painful muscles — but the long-term change comes from retraining the way your body moves.That’s why, at JSR, dry needling is paired with:Corrective strength trainingMobility and stability workEducation on movement and load managementSport-specific rehab
The goal isn’t to “chase pain.”
The goal is to address the root cause so you can get back to the activities you love.Who Can Benefit?
Dry needling may be helpful if you are:An athlete dealing with recurring tightnessAn active adult dealing with work-related painReturning from injury and struggling with muscle tensionDealing with chronic pain that hasn’t improved with stretching alone
If you’re unsure whether it’s right for you, a physical therapist can evaluate your movement, strength, and symptoms first.If you’re looking for dry needling or sports-focused physical therapy in Winter Springs, Winter Park, Orlando, or surrounding Central Florida areas, we’d love to help.Our one-on-one approach ensures every session is tailored to you — not a template.Schedule an evaluation to find out whether dry needling may help reduce your pain, improve mobility, and get you back to moving comfortably again.Pickleball Injury Risks & Player Demographics: What Athletes Should Know

Pickleball has exploded in popularity in recent years, drawing players from all age groups and fitness levels. While it’s a fun way to stay active and social, the sport does carry a notable risk of injury — especially for certain age groups and competitive levels. Understanding the statistics and common injury trends can help players stay safer and enjoy the game for years to come.Why Injury Risk Is Rising
Pickleball-related injuries in the United States have increased substantially over the last decade as more people take up the sport. From 2013 to 2022, the number of pickleball injuries presenting to U.S. emergency departments jumped dramatically, with tens of thousands of players seeking care each year. In 2022 alone, about 13,690 pickleball-related injuries were estimated in U.S. emergency departments — a dramatic rise compared with earlier years.
PMC
Research also shows injury numbers increased sharply during the pandemic years, likely due to more people playing recreational sports and expanding participation across age groups.Who Is Getting Hurt?
One of the most consistent findings in pickleball injury data is the age distribution of players who get injured: A large majority of pickleball injuries occur in players aged 50 and older, with some studies finding that 87–90% of emergency room visits for pickleball injuries involve adults over 50.National injury surveillance data also show that most injury cases occur in players between 60 and 79 years old, reflecting both the popularity of pickleball among older adults and age-related physical risks.It’s worth noting that while older players tend to represent the highest numbers of injuries, middle-aged and younger adult players still face significant risk, especially if playing frequently or without proper preparation. One study found injury prevalence ranged from nearly 50% in younger adults (18-32 years) to over 77% in 48-62-year-olds.
What Types of Injuries Are Most Common?
1. Acute injuries
– Fractures and falls are surprisingly common, especially among older players. Several injury datasets report fractures making up around 27-30% of pickleball injuries, particularly wrist and upper extremity fractures.2. Soft-tissue injuries
– Sprains, strains, and muscle injuries are also frequent, particularly involving the legs and ankles — likely due to quick lateral movements and sudden stops typical of pickleball play.Other injury types include shoulder and elbow issues (“pickleball elbow”), Achilles and knee injuries, and even eye injuries — with over 1,200 pickleball-related eye injuries reported in one recent study.Why These Injuries Happen:
Injury risks in pickleball aren’t random — they stem from a combination of factors:Sudden and multi-directional movements: Quick lateral shuffles and abrupt stops can stress joints and soft tissue.Falls: Loss of balance or unexpected slips are very common, especially on uneven surfaces or in older adults.Repetitive motion: Repeated swings and cutting movements can overload muscles and tendons over time.Lack of preparation: Many players skip adequate warm-ups, strength work, or mobility training — increasing risk.
These factors underscore why proper physical preparation and recovery are essential for pickleball longevity.Average Player Age Matters
Although specific national surveys vary, pickleball’s player base has been trending younger as the sport spreads. According to industry reports, millions of Americans now play pickleball — and the average player age has been reported in the mid-30s, reflecting its growing appeal beyond traditional “senior sport” demographics.However, even when the average age includes many younger players, injury risk remains disproportionately high among older adults, largely due to age-related changes in balance, bone density, and muscle strength.What This Means for You
Pickleball can be an excellent way to stay fit and active at any age. At the same time, awareness of injury risk is critical. Knowing the trends — such as higher injury rates in older players and common fracture and sprain patterns — helps players and clinicians alike make smarter training choices.
Physical therapists can play a key role in injury prevention and recovery, focusing on:Strength and balance trainingMovement mechanics and injury reduction strategiesWarm-up, cool-down, and recovery protocols
If you experience pain during or after pickleball play, or if you want a personalized training plan to reduce your injury risk, consider consulting a sports-focused physical therapist — especially before symptoms become more serious.When “Tight Muscles” Are Actually Weak
Why Stretching Isn’t Always the Answer
Feeling tight is one of the most common complaints we hear in physical therapy. Tight calves, hips, hamstrings, shoulders, or low backs often lead people to stretch more and more, hoping for lasting relief.I personally hear this all of the time regarding the hamstrings. And, in most cases, I find that a lot of these patients have good hamstring flexibility which my patients are shocked to hear.So what does it mean when a feeling of muscle tightness isn't a flexibility problem?In many cases, a muscle feels tight because it is weak, fatigued, or unable to handle the demands placed on it. And when weakness is the real issue, stretching alone rarely solves the problem long-term.Why Muscles Feel Tight in the First Place
Muscle tightness is not always about lack of length. It can be a protective response from the nervous system.When a muscle lacks strength, endurance, or control, the body may increase tension in that area to create a sense of stability. This makes the muscle feel stiff or restricted, even though it may not actually be shortened.This is especially common in active individuals who train frequently, sit for long hours, or return to activity after injury.3 Signs Your “Tightness” May Actually Be Weakness
1. Tightness Gets Worse With Activity
True muscular stiffness often improves once you warm up. If a muscle feels progressively tighter, more fatigued, or more uncomfortable during workouts or sports, it may be struggling to keep up with the load being placed on it.Weak muscles often tighten as a protective mechanism when they are being overworked.2. The Same Muscle Feels Tight After Every Workout
If you constantly feel tight in the same area after every training session, run, or game, flexibility is unlikely to be the main issue.Recurring tightness in the same spot often means the muscle lacks the strength or endurance required for your activity, causing it to fatigue quickly and tighten repeatedly.3. Stretching Only Provides Short-Term Relief
If stretching helps for a few minutes or hours but your tightness quickly returns, this is a strong clue that stretching alone is not addressing the root cause.Stretching can temporarily reduce tension, but it does not increase load tolerance or control. When a muscle is weak, the sensation of tightness often returns as soon as you begin moving again.Why Stretching Alone Doesn’t Fix Weakness
Stretching is a useful tool and can be useful temporarily (while you are addressing muscle weakness,) but it doesn’t improve strength, stability, or movement control.If a muscle cannot handle the demands of your sport, workouts, or daily activities, it will continue to tighten no matter how much time you spend stretching. Over time, this can lead to:Ongoing discomfort or stiffnessRecurrent injuriesReduced performanceCompensations in nearby joints or muscles
Without addressing strength and movement, tightness often becomes a recurring cycle.When Strengthening Is the Missing Piece
Targeted strengthening helps muscles:Tolerate load more efficientlyImprove coordination and enduranceReduce unnecessary tensionSupport joints more effectively
When strength and control improve, muscles often stop “guarding,” and the sensation of tightness naturally decreases — sometimes without additional stretching at all.This is why many people feel looser and better after consistent strengthening, even if they stretch less.When adding strengthening to address weakness, make sure to hit each problem muscle 2-3x/week for 2-3 sets of anywhere between 8-15 reps.Why Proper Assessment Matters
Not all tightness needs stretching. Sometimes it needs strengthening.Determining which approach is appropriate requires evaluating strength, movement patterns, joint mobility, and how your body responds to activity. Treating every tight muscle the same way can lead to frustration and stalled progress.A physical therapist can identify whether tightness is coming from true mobility restrictions, muscle weakness, or movement inefficiencies — and create a plan that actually addresses the cause.The Hidden Cost of “Playing Through” an Ankle Sprain
Why Rest & Recovery Matter
An ankle sprain is one of the most common injuries in sports — and one of the most ignored.An ankle sprain occurs when the ligaments that support the ankle joint stretch or tear — often from a twist, awkward landing, or sudden change in direction. While it might be tempting to “tough it out,” especially for athletes or dedicated weekend warriors, skipping proper recovery can have long-term consequences.Many athletes treat it like a minor inconvenience: tape it, lace up tight, and keep playing. While that mentality might feel tough in the moment, playing through an ankle sprain without proper rest and recovery can lead to long-term problems that are far harder to fix than the original injury.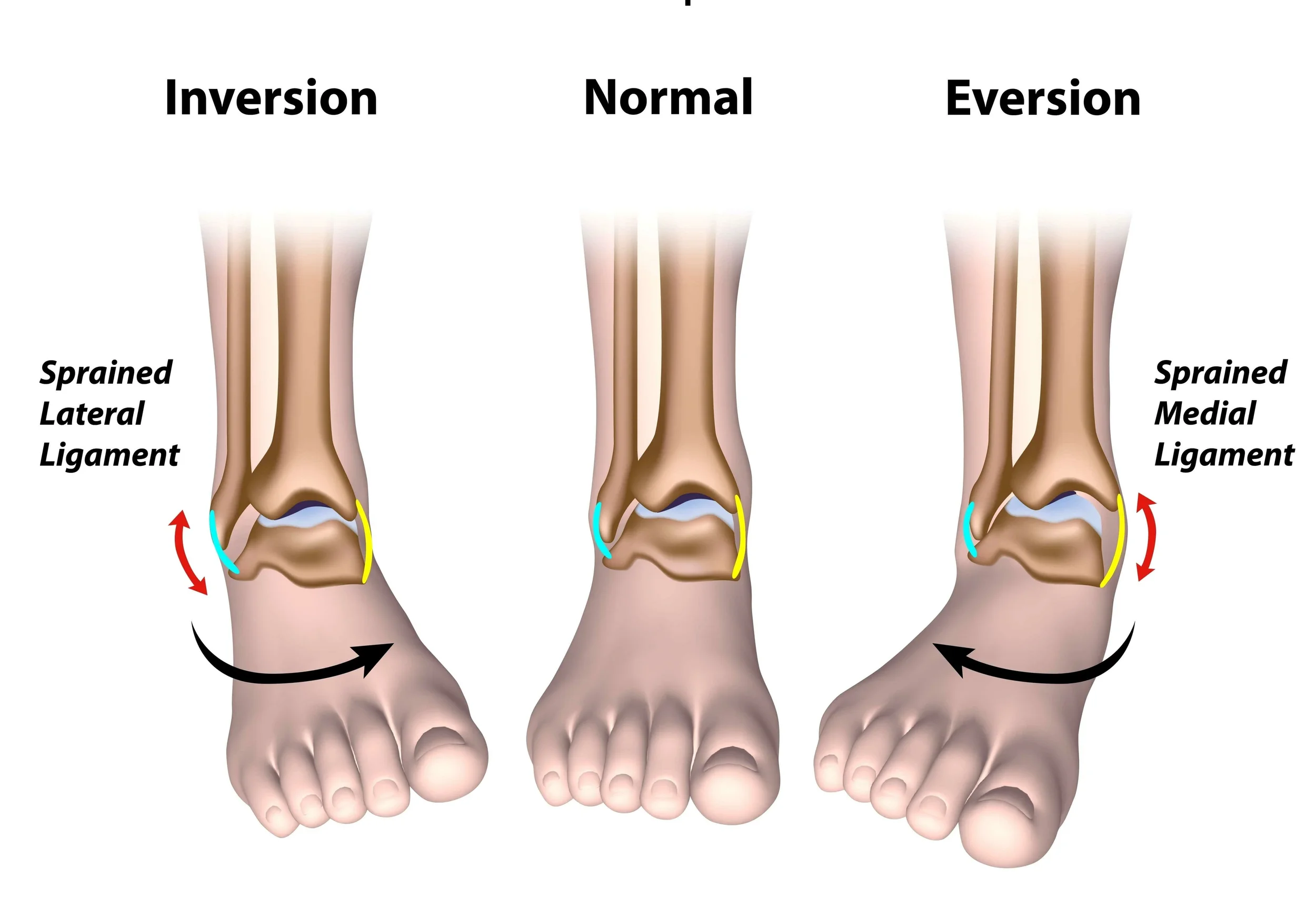
Most Common Sports for Ankle Sprains (and Why Athletes Are at Risk)
Ankle sprains are especially common in sports that involve jumping, rapid changes of direction, cutting, or contact — movements that stress the ankle joint repeatedly or unpredictably.Here are some of the top sports and statistics:
Basketball consistently shows among the highest ankle-sprain rates. In one study, the ankle-injury rate was ~3.85 per 1,000 participations.Soccer is frequently listed among the top sports for ankle sprains, due to cutting, pivoting, and contact.Volleyball players face higher ankle sprain risk (especially high ankle-sprain risk vs the traditional inversion ankle sprain) because of jumping and landing, especially at the net.Indoor/court and team sports broadly (handball, field hockey, netball, etc.) — A broad review found that ankle sprains are among the most common injuries across many sports — particularly those involving court play, quick direction changes, or jumping.
At the collegiate level, foot and ankle injuries (with ankle sprains the most common) often account for a substantial portion of all injuries — especially in disciplines involving jumping and changes in directionBecause athletes in these sports frequently push through minor injuries or “shake off the pain” to keep playing, ankle sprains often go under-treated — which can lead to a cascade of future problems.Long-Term Implications of Skipping Proper Recovery
Neglecting recovery or returning to sport too early after an ankle sprain can lead to several negative long-term outcomes:Chronic Ankle Instability (CAI): Up to ~20% of people who suffer an acute ankle sprain go on to develop CAI; other studies suggest recurrent sprains and persistent symptoms in 40–70% of cases.With CAI, the ankle can repeatedly “give way,” leading to further sprains, swelling, and functional limitations.Post-traumatic osteoarthritis (PTOA): Repeated or poorly healed sprains can cause joint cartilage damage, early wear and tear, and eventual arthritis — even in relatively young athletes.Altered biomechanics, secondary injuries: To compensate for a weak or unstable ankle, people often change their gait or movement patterns — which can overstrain other joints (knees, hips, back) or lead to chronic stiffness in the ankle.Reduced performance & quality of life: Chronic pain, instability, or limited mobility can interfere with athletic performance, daily activities, and long-term physical health.
How Proper Recovery + Rehab Helps:
Allows ligaments to heal properly — Controlled rest, protection (bracing or limited weight-bearing if needed), and gradual rehab give the injured ligaments time to scar in and regain strength.Restores stability and proprioception — Rehab should include exercises for range of motion, strength, balance, and neuromuscular control. This is crucial for preventing re-sprains or instability.Prevents chronic issues — By allowing proper healing and retraining the supporting muscles/joints, you significantly reduce risk of chronic instability, arthritis, and long-term impairment.Prepares you safely for return to sport or activity — Rather than jumping back in too soon and risking re-injury, a full recovery gives you the best chance of returning at full strength with reduced long-term risk.
An ankle sprain may seem like a short-term setback, but how it is managed early can greatly influence long-term movement, performance, and joint health. Allowing the ankle to fully recover helps restore strength, stability, and confidence while reducing the risk of future injuries. Working with a physical therapist ensures that recovery focuses not only on pain relief, but on rebuilding proper movement and preparing the body for a safe return to sport or daily activity.Why Grip Strength Matters in Baseball Players

Grip Strength: The Secret Link to Velocity, Control & Shoulder Health
Grip strength might be the simplest but most overlooked metric in overhead athletes — especially baseball players.It predicts shoulder stability, elbow stress, velocity, and even how efficiently energy transfers through the throwing chain.Overhead athletes generate enormous force through the kinetic chain — from the ground → hips → torso → shoulder → elbow → wrist → hand.The hand is the final link in that chain.If grip strength is low or imbalanced, the entire chain becomes less efficient… and less safe.So How Exactly Does Grip Strength Help?
1. Grip Strength = Shoulder Stability
During throwing, the rotator cuff fires intensely to stabilize the humeral head.
But research in biomechanics shows that distal stability (forearm & grip) reduces proximal load.
Stronger grip =More co-contraction of rotator cuffBetter humeral head controlImproved dynamic stabilityLess stress on the labrum and capsule
A stronger grip helps protect the shoulder during high-velocity throwing.2. Grip Strength Correlates With Velocity & Control
A stronger grip improves:Wrist stiffnessEnergy transfer at ball releaseSpin rate & command
Pitchers with higher grip strength often demonstrate:Higher velocityMore stable release pointReduced elbow varus torque
3. Grip Strength Protects the Elbow (UCL)
UCL stress peaks during late cocking and acceleration. A strong grip improves forearm flexor-pronator activation — the natural dynamic protectors of the UCL.Low grip strength = increased UCL load = higher injury risk.How Can We Test Grip Strength:
We typically test grip strength using a device called a dynamometer. These devices can be inexpensive with some $30 options on amazon. It is ideal to test grip strength in 2 positions:Arm at the side of the body with the elbow bent to 90degreesArm straight overhead
To determine left to right grip strength you take 3 maximal effort squeezes of the dynamometer in each position on each hand. Add the 3 numbers together then divide by 3 to get the average in each position. You can then compare these measurements left to right and overhead to down at the side of the body.
Why Test Grip Strength Overhead?
Testing overhead simulates the functional throwing position where the shoulder is externally rotated and elevated — the exact moment when:Rotator cuff demand is highestGrip-forearm-shoulder linkage matters mostInjuries frequently occur
The Key Rule: Grip Strength Overhead Should Be ~2% Stronger Than at the SideBecause in overhead position the rotator cuff and scap stabilizers engage more. This increases neuromuscular drive through the kinetic chain → producing a small but measurable strength boost.The 2% Rule
If overhead grip strength is roughly 2% stronger than grip at the side → NORMALIf overhead grip = SAME or WEAKER → Red flagPossible cuff inhibitionScapular dyskinesisPrevious shoulder or elbow irritationPoor energy transferIncreased injury risk
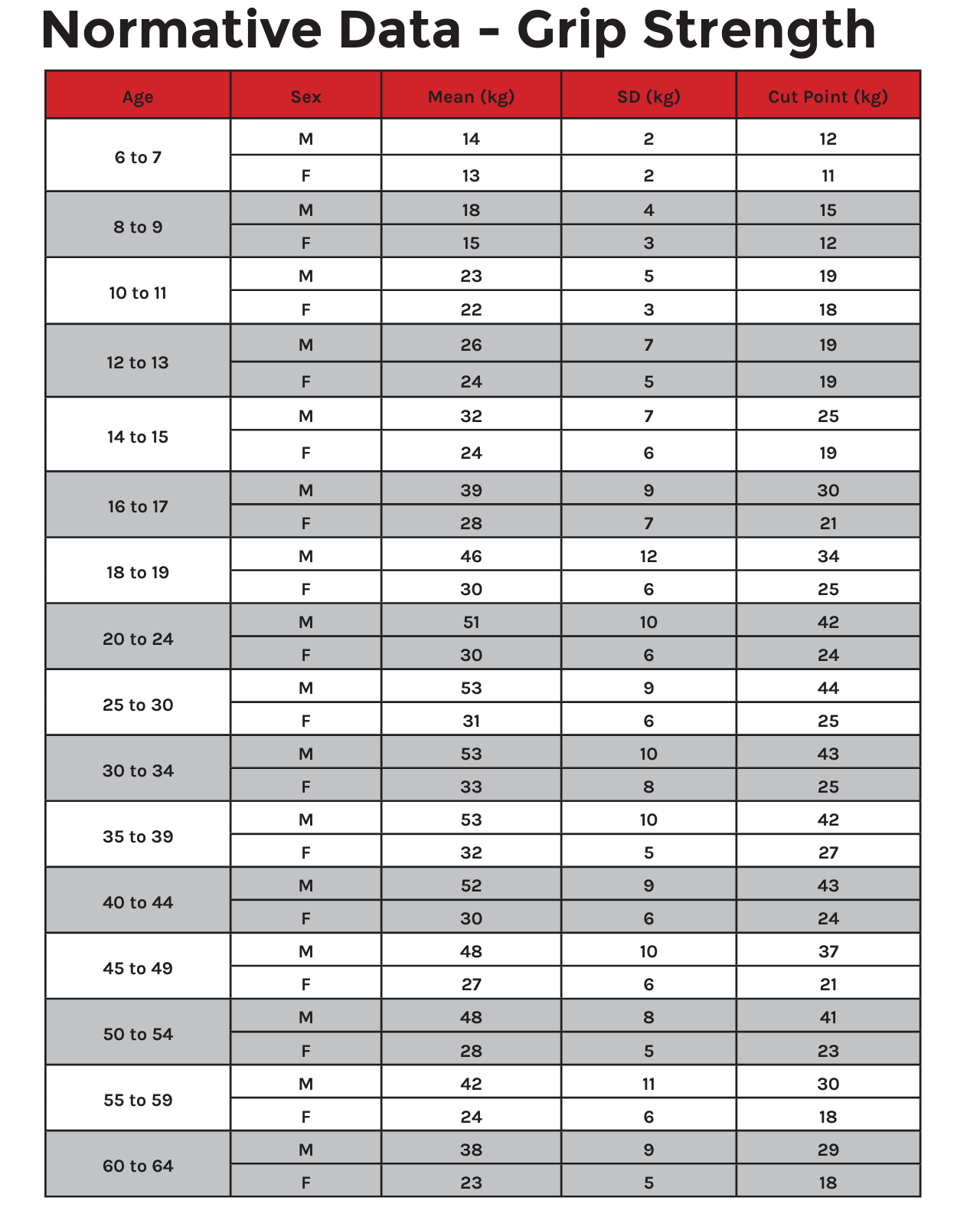
Normative Grip Strength Values: Provided through FMS
The Grip testing mentioned above is just one of many tests we perform on our baseball players to ensure that the whole body is functioning cohesively as a unit. There are many other body parts to look at to ensure too much stress isn't going to the elbow or shoulder such as hip mobility, core strength, pelvic control, single leg balance and strength, etc.
And I know we focused on Baseball, but grip strength is important in all overhead sports whether its volleyball, tennis, pickleball, football, etc.
If you would like to be screened due to pain or a history of pain, let us know!Shoulder Injuries in Swimmers — What Every Swimmer & Coach Should Know

Swimming is a fantastic sport for cardiovascular fitness, endurance and whole-body conditioning. But despite being low-impact on joints compared to many land sports, swimmers face very high rates of shoulder problems. Because every stroke uses the shoulder repeatedly — often thousands of times per week — subtle overload, technique flaws or muscle imbalances can add up.At JSR, we see many swimmers with shoulder pain, and it’s our goal to help you recognise, prevent and manage these injuries so you can stay in the pool strong and pain-free.How common is shoulder pain/injury in swimmers?
A recent systematic review found reported rates of shoulder injuries among competitive swimmers between 40% and 91%, depending on study design, age and competitive level. MDPI+2journal.aspetar.com+2In a survey of youth swimmers aged 9-17 in the U.S., 49% reported shoulder symptoms that impacted their swimming. PMC+1One 2014 article stated that shoulder injuries are the most common injuries in swimming, with prevalence in many studies from 47% to 90%. journal.aspetar.comAmong highly trained swimmers, one study reported 74% had experienced at least one shoulder injury, and more than half of those had a recurrence. British Journal of Sports Medicine
The takeaway: shoulder issues are very common in swimmers, not just the occasional problem. Recognising the risk and taking proactive steps is key.Why do swimmers get shoulder injuries so often?
Here are some of the major contributing factors:Repetitive overhead motion – Freestyle, butterfly and backstroke all involve repeated overhead or near-overhead arm movements, putting the shoulder in vulnerable positions for long periods. journal.aspetar.com+1High training volume – Elite swimmers sometimes complete thousands of arm rotations per day. That repeated load accumulates. PMC+1Technique flaws – Small inefficiencies in stroke mechanics (for example poor body roll, incorrect entry, hand path) can increase shoulder stress. journal.aspetar.comMuscle imbalances / fatigue – If the shoulder stabilisers (scapular muscles, rotator cuff) are weak or fatigued, then the larger muscles take over and strain increases.Training load spikes – Rapid increases in volume or intensity (new sets, more distance, hand paddles or drag devices) are often tied to onset of pain. journal.aspetar.com+1Prior injury – A history of shoulder pain is one of the strongest risk factors for new or recurring shoulder injury. PMC+1
The most common shoulder injuries in swimmers:
1. Swimmer’s Shoulder (Overuse Impingement)
Often called “swimmer’s shoulder,” this is really a pattern of overload, irritation or impingement of the rotator cuff tendons (especially the supraspinatus) and related structures. The term is broad but useful.
journal.aspetar.com
+1
What to look for: Pain with the catch or pull phase of stroke, soreness after training, sometimes pain in daily life if it’s progressed.
2. Rotator Cuff Tendinopathy / Tendinitis
With constant repeated motion, the rotator cuff (the small stabilising muscles of the shoulder) can develop tendon irritation or degeneration. Over time it can become a chronic issue rather than an acute tear.
Key issues: Weakness in external rotation, pain with resisted movements, fatigue of the shoulder late in training.
3. Labral Injuries (e.g., SLAP tear)
The labrum is the ring of cartilage around the shoulder socket; in some swimmers, repeated overhead stress or subtle instability can cause fraying or tearing of the labrum.
Signs: Deep-shoulder pain, catching or clicking, decreased power in strokes, sometimes a feeling of looseness.
4. Shoulder Instability / Multidirectional Instability
Some swimmers develop too much laxity or movement in the shoulder joint (often because of high training loads + technique demands) which leads to pain, micro-trauma and inefficient mechanics.
What you might notice: Shoulder “slipping” sensation, fatigue when doing long sets, uneven stroke power.
5. Scapular Dyskinesis
The shoulder blade (scapula) must move smoothly to allow the arm to move efficiently overhead. When the scapula is not stable (dyskinesis), the shoulder joint takes extra loads.
Clinical clue: Asymmetry in the shoulder blade during movement, difficulty holding proper body roll or stroke posture, fatigue of shoulder stabilisers.How can swimmers and coaches address/prevent these injuries?
Here are practical tips to help avoid shoulder problems — and to manage them early if they arise.
Monitor training load – Avoid large sudden increases in volume or intensity. Gradual progression is safer.
Technique check – Regularly review stroke mechanics: hand entry, catch, pull-through, recovery, body roll. Poor mechanics = more shoulder stress.
Strength and conditioning – Emphasise rotator cuff strength, scapular stabilisation, core and trunk control. A balanced dryland program helps.
Scapular control – Exercises like scapular retractions, stabiliser work, serratus anterior strengthening are helpful.
Flexibility / mobility – Ensure adequate range of motion in the shoulder, thoracic spine, and control of the shoulder blade.
Early recognition – If a swimmer reports shoulder soreness that’s lingering, catching, or increasing during training—address it early rather than ignore it.
Load modification – If pain occurs, reducing volume, avoiding aggravating sets, and cross-training can prevent escalation.
Multi-disciplinary approach – Work with coaches, swim technique experts, strength & conditioning and physical therapy together for best results.When to see a physical therapist?
If you're a swimmer and experiencing:Persistent shoulder pain (that doesn’t go away after rest)Loss of stroke power or speed related to the shoulderClicking, catching, or instability in the shoulderRecurring shoulder issues
…then it’s a good idea to have an evaluation by a physical therapist experienced with swimmers. At JSR we assess shoulder strength/motion, scapular control, and work with you and your coach to build a targeted plan.Shoulder injuries in swimmers are common but not inevitable. With smart training, good technique, strength & mobility work, and early attention to symptoms, most swimmers can perform and train without chronic shoulder pain.At JSR, we aim to help you stay strong, efficient and injury-free in the pool. If you’d like a shoulder screening, or want to discuss swim-specific shoulder rehab, we’d be glad to help.How to Tackle the Aging Knee: What to Know about Arthritic Knee Pain

As we get older, our knees take a lot of wear and tear. One of the most common culprits behind knee pain is Knee osteoarthritis (knee OA) — a form of arthritis that affects the cartilage, bones, and other structures of the knee joint. In this post we’ll walk through what it is, why it happens more with age, who is most affected, and what you can do (with your physical therapist!) to feel better and stay active.What is Arthritic Knee Pain?
Knee osteoarthritis happens when the protective cartilage in the knee gradually wears down. This leads to changes such as:Bones rubbing or bumping each other,The joint lining becoming inflamed,Possible bony outgrowths (osteophytes), andStiffness, swelling and pain in and around the knee.
This doesn’t happen overnight — it’s a slow process, often over many years. It becomes more likely as we age, especially if we’ve had prior knee injury, are carrying extra weight, or have certain structural knee alignment issues.Why Age Matters
Age is one of the biggest risk factors for knee OA. Here are some key statistics:Globally, the prevalence of knee OA in people aged 15 and over is about 16.0%, and for those aged 40 and over it rises to about 22.9%. PMCAccording to the World Health Organization, about 73% of people with osteoarthritis are older than 55 years, and around 60% are female. World Health OrganizationIn the U.S., about 9.3% of the population is diagnosed with symptomatic knee OA by age 60. PMCAmong adults aged 45-64 in the U.S., symptomatic knee OA affects roughly 7.8% of people; for those over age 65 it rises to about 15.6%. PMCThe annual incidence (new cases) of knee OA is highest in the 55-64 age group. Osteoarthritis Action Alliance+1
In simple terms: as you cross into your 50s and beyond, the risk of developing knee osteoarthritis goes up significantly. The wear-and-tear over years, combined with factors like previous injuries, activity level, body weight, and genetics, all add up.Who is Most Affected?
While knee OA can occur in younger adults — especially if they’ve had knee injuries or are obese — the “aging” population is more commonly impacted. Some patterns to note:Women are at higher risk than men in many studies. PMC+1People who are overweight or obese have a higher risk (because extra weight increases the load on knee joints). BioMed Central+1The average/median age of diagnosis of symptomatic knee OA in one U.S. study was about 55 years. PMCAlthough older age groups have higher percentage prevalence, because there are many people in the 45-64 age range, the number of people with knee OA in that age band is nearly as high as older groups. PMC
For a physical therapy practice, this means many patients in their 50s, 60s and older will likely start showing knee pain from arthritic changes — but they don’t have to just accept it.What Does Knee Arthritis Feel Like?
In the clinic you may see patients describing:Gradual onset knee pain (often worse after activity or long periods of standing)Stiffness in the morning or after sitting for a whileDifficulty going up or down stairsA “giving way” or instability feeling (due to weakened muscles or altered joint mechanics)Possible swelling, warmth, or a “grating” feeling inside the knee
Because the condition progresses slowly, patients may attribute the symptoms to “just getting older.” It’s important to recognize that — yes, age is a factor — but there are things we can do to slow progression and improve function.How Physical Therapy Can Help
1. Strengthening & Muscle Support
Stronger muscles around the knee (quadriceps, hamstrings, glutes) take pressure off the joint and help improve alignment and movement patterns.2. Improving Mobility & Joint Mechanics
Gentle motion, stretching, and activity modification help maintain joint mobility so the knee doesn’t lock up or worsen stiffness.3. Activity Guidance
We’ll help patients stay active (which actually helps cartilage health) while avoiding movements that overload the knee. Low-impact aerobic work, proper footwear, and safe stair/step mechanics all matter.4. Weight & Load Considerations
A study found that for every 5lbs of fat, the load on the knee joint increases by 4lbs. So by losing even just 10lbs, it takes roughly 40lbs of pressure off of the knee joint.5. Education & Pain Management
Teaching patients about proper biomechanics, pain-relieving strategies, and strategies to avoid worsening the joint helps them stay in control.Age Groups & What to Know:
Here’s a breakdown of age bands and what to watch for:40-49 years: Some early arthritic changes may begin. Prior knee injuries, high impact sports, obesity matter. Early intervention is beneficial.50-64 years: This is often the “sweet spot” for diagnosis of symptomatic knee OA. Pain may become more noticeable, especially with stairs, walking, prolonged standing.65 years and older: Higher prevalence of knee OA; however, because of other comorbidities (balance issues, bone health, other joints), tailored rehabilitation is critical to maintain independence and mobility.
Key Take-Home Messages
Arthritic knee pain is very common in older adults — age 55 and up is where we start to see the bulk of diagnoses.You’re not just “old and sore” — knee osteoarthritis is a real joint condition that responds to intervention.Physical therapy is not too late at any age — strengthening, mobility work, load management and activity guidance can improve quality of life.The earlier you engage (even if symptoms are mild), the better chance you have of slowing progression and maintaining an active lifestyle.Age matters as a risk factor, but individual risk also depends on weight, injury history, activity level, and muscle strength/conditioning.
And to the active adults who still want to train like they did when they were younger— the key is finding the right volume that works for you. I personally used to play soccer everyday. But as I have gotten older, and my own personal knee arthritis has started to set in, I found that two days a week of soccer was doable without flaring up my knees. I also strength train and stretch at least 2 days per week to ensure my joints are protected when I step on the field. Sometimes figuring out the “right”" amount of volume takes some trial and error, but it is definitely possible with smart choices and discipline. Maybe it’s as simple as running 3 miles instead of 4 because you notice at 3.5-4 miles your knees ache for days. And instead of running daily you can choose to run every other day and supplement biking for extra cardio. These are all decisions we can help you with so feel free to reach out with any questions! Average Return‑to‑Sport Times After ACL Surgery: What the Research Really Shows
When athletes injure their ACL (anterior cruciate ligament), one of the first questions is: "How long until I can play again?" The honest answer is: it depends – but we have excellent research to help guide expectations…
When athletes injure their ACL (anterior cruciate ligament), one of the first questions is: "How long until I can play again?" The honest answer is: it depends – but we have excellent research to help guide expectations.The ACL is one of the key stabilizing ligaments in the knee, helping control rotation and preventing the shin bone from sliding forward. It is most often torn during sudden cutting, pivoting, or landing movements — especially when the foot is planted and the knee twists inward. Non‑contact injuries (like a quick change of direction or awkward landing) make up the majority of ACL tears in field and court sports.Below is a current look at what return-to-sport timelines look like today:The "6‑Month" Myth vs. Reality
Years ago, many athletes were told that they could return as early as six months after ACL reconstruction. Today, we know that rushing back too soon significantly increases the risk of re‑injury.
Modern research shows that athletes who return before 9 months are up to 7 times more likely to tear their ACL again.
Differences by Sport:
Sports involving jumping, cutting, and pivoting — such as soccer, basketball, lacrosse, football, and tennis — typically require 9–12+ months before a safe return.
Linear sports like running or cycling may allow earlier return, often between 6–9 months, depending on symptoms and strength recovery.
Why "time alone" isn’t enough:
Return‑to‑sport decisions today are based on criteria, not just the calendar. Common clearance factors include:Quad and hamstring strength symmetry (90% or greater)Balance and landing mechanicsSingle‑leg hop testingConfidence and psychological readinessMovement quality in cutting/jumping
Psychological Readiness Matters Too
Research shows that fear of re‑injury is one of the most common reasons athletes delay returning to sport—even when physically cleared. Structured rehab that includes confidence‑building and sports‑specific progressions leads to better outcomes.Key Takeaways:
Most athletes safely return to sport between 9–12 months after ACL reconstruction.Returning before 9 months dramatically increases the risk of re‑injury.A full clearance is based on performance criteria, not just the date on the calendar.Strength, control, and confidence are just as important as ligament healing.
If you’re recovering from ACL surgery or working your way back to your sport, a physical therapist can guide every phase of your rehab and testing so you return not only faster — but safer.Research Sources:
Grindem et al. "Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction." British Journal of Sports Medicine, 2016.
Beischer et al. "Young athletes who return to sport before 9 months after ACL reconstruction have a higher risk of reinjury." American Journal of Sports Medicine, 2020.
Ardern et al. "2018 International Olympic Committee (IOC) consensus statement on return to sport after injury." British Journal of Sports Medicine, 2018.
Understanding Frozen Shoulder
Frozen shoulder, also called adhesive capsulitis, is a painful condition that limits motion in the shoulder joint. It occurs when the capsule of connective tissue surrounding the shoulder thickens and becomes tight...
Frozen shoulder, also called adhesive capsulitis, is a painful condition that limits motion in the shoulder joint. It occurs when the capsule of connective tissue surrounding the shoulder thickens and becomes tight. This reduces the smooth gliding movement of the joint and makes even simple daily activities difficult, such as reaching overhead or behind the back.This condition affects an estimated two to five percent of the general population. It is more common in adults between the ages of forty and sixty and is seen more often in women than in men. People with diabetes are at a much higher risk. Research shows that as many as twenty percent of people with diabetes will develop frozen shoulder at some point.Frozen shoulder usually develops in stages and may take many months to improve.How Long Does Frozen Shoulder Last
Frozen shoulder is temporary. The process usually lasts from one to three years, though many people begin feeling better much sooner once motion improves and the irritation settles. With consistent therapy and proper pacing, the shoulder often regains strength and mobility far earlier than the complete timeline suggests.
Common symptoms include:
Deep aching pain in the shoulder
Stiffness and loss of motionDifficulty sleeping because of shoulder discomfortWeakness due to pain and guarding
The pain is often constant and can worsen at night. Over time, the joint becomes more restricted which limits normal movement during daily tasks. These symptoms are frustrating, but they are reversible and can respond well to guided care.The Three Phases of Frozen Shoulder
Frozen shoulder develops in a predictable pattern. Understanding the stages helps patients stay encouraged during treatment.Freezing Phase: Pain begins gradually and motion becomes limited. The shoulder feels stiff and irritated. This is when calming the joint is most important.Frozen Phase: Pain often begins to lessen, while stiffness remains the main concern. Many people begin to feel small gains in comfort during this period.Thawing Phase: Movement steadily improves and the shoulder becomes more flexible. This is the stage where patients often feel major progress and return to confident use of the arm.Why Hyperirritability Matters in Physical Therapy:
Many patients with frozen shoulder experience what therapists call a hyperirritable shoulder. This means the tissues react strongly even to gentle stretching or light pressure. Because of this, pushing too hard can increase pain and slow progress.
A thoughtful approach to physical therapy is important. Treatment often focuses first on calming the irritated tissues through gentle movement, soft tissue work, and pain control strategies. Only after the irritation settles can more aggressive stretching be introduced. Physical therapy that accounts for tissue irritability of the shoulder responds better and recovery tends to move forward more smoothly.It is very important to not just push through pain. If you are noticing that your shoulder pain and stiffness is worse that night or the next day following stretching/exercises, than you need to go lighter with your program. Non Surgical Treatment Options:
Most people improve with non surgical care. These treatments includePhysical therapy to restore motion, strength, and joint mobilityTargeted stretching taught in a gradual and safe mannerHeat or cold for pain reliefJoint mobilization performed gently by a licensed therapistAnti inflammatory medication when recommended by a medical providerCorticosteroid injections in some cases to calm inflammation
With committed participation many patients see significant improvement in function over time without the need for an operation.Surgical Treatment Options:
If pain and stiffness remain severe and do not improve after several months of therapy, a physician may recommend a surgical option. The two most common procedures areManipulation under anesthesia, where the doctor gently moves the shoulder to loosen the tight capsuleArthroscopic capsular release, where tight tissue is carefully trimmed to restore motion
Even after surgery, physical therapy remains an important part of recovery to maintain the gains in mobility and to retrain healthy shoulder movement.The Outlook:
The outlook for frozen shoulder is encouraging. The body is built to heal this condition and the great majority of people regain comfortable function. With patience, proper pacing, and skilled therapy, daily activities become easier and confidence in the shoulder steadily returns. Progress sometimes feels slow early on, but it builds momentum as the shoulder moves from stiffness toward freedom of motion.Why Ankle Sprains Are the Most Common Sports Injury — and How to Recover Stronger
Whether you’re playing basketball on the court, sprinting down a soccer field, or diving for a volleyball save — your ankles are doing a lot more work than you think. In fact, ankle sprains are the single most common injury in sports, accounting for up to 40% of all athletic injuries worldwide.
Recent studies show that athletes in court sports like basketball and volleyball face the highest risk — often more than 5 sprains for every 1,000 games or practices. Field sports such as soccer and football aren’t far behind, with frequent twists, tackles, and uneven turf contributing to steady injury rates year after year.
Once you sprain an ankle, your odds of doing it again increase. Research suggests that nearly 1 in 5 athletes will experience recurrent sprains or develop chronic ankle instability, leading to ongoing weakness, swelling, or “giving way.”
But here’s the good news: understanding which sports carry the highest risk helps athletes, coaches, and clinicians focus on prevention — from strength and balance training to proper taping/footwear.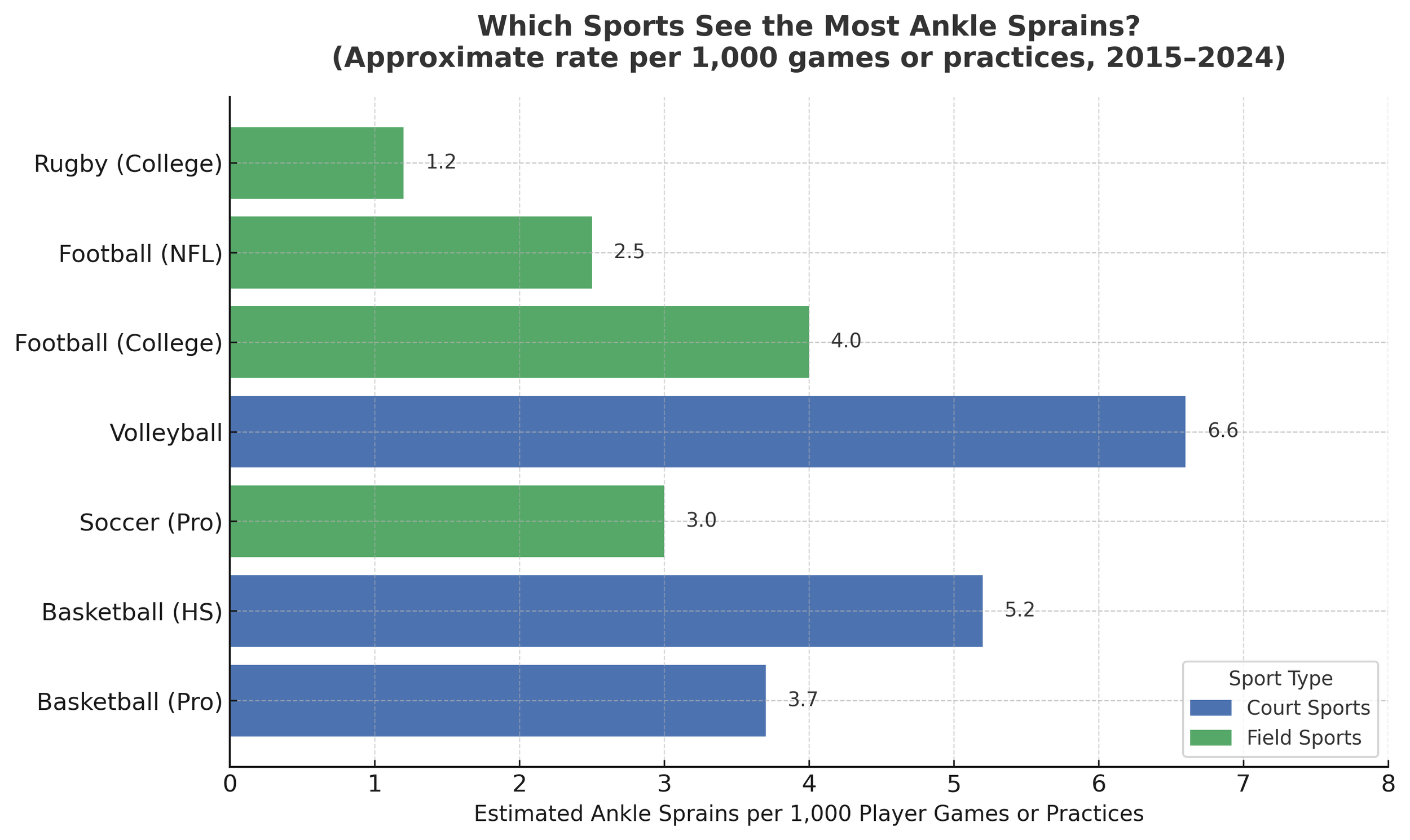
What These Numbers Mean for You
The chart above isn’t just about numbers — it’s about how your sport stacks up in ankle risk and what that means for keeping you on your feet.Court sports (like basketball and volleyball) lead the pack for ankle sprains because of the constant jumping, cutting, and landing on other players’ feet. Quick direction changes and rebounds make these sports a perfect storm for rolled ankles.Field sports (like soccer, football, and rugby) cause more contact-related ankle injuries — think awkward tackles, slippery grass, and high-velocity collisions. These injuries often involve the syndesmosis (“high ankle”) and can sideline athletes longer.Repetition matters: The more you play, the higher your exposure risk. That’s why professionals and year-round athletes report higher rates than casual players.Prevention pays off: Studies consistently show that ankle braces, taping, and neuromuscular training can cut sprain rates by 40–50%.Rehab isn’t optional: Once you’ve sprained an ankle, skipping rehab doubles your chances of another injury — and long-term instability can linger for years.
Bottom line: No matter your sport, ankle strength and balance training aren’t just accessories — they’re your best defense against the most common injury in athletics.
Every ankle sprain tells a story — but at our clinic, we make sure it doesn’t become a recurring chapter. While most people think a sprain just needs rest and time, research shows that without proper rehab, up to 70% of athletes develop lingering weakness or instability. That’s where physical therapy makes the difference.At our facility, recovery isn’t a one-size-fits-all process. We combine evidence-based rehab with sport-specific retraining to restore balance, strength, and movement confidence — so you can return not just to play, but to peak performance.How We Address Ankle Sprains In Physical Therapy:
Early Phase: Calm the Injury, Set the Foundation
In the first stage, our priority is to reduce swelling, relieve pain, and restore gentle motion. We also strengthen the joints and muscles above the ankle — the hips, knees, and core — to keep your body balanced during recovery.
We introduce light neuromuscular and proprioceptive training early to keep your ankle connected to your brain’s balance system.Treatments that accelerate this phase include:MyACT Piezowave therapy (shockwave treatment) to boost circulation and healing.Targeted massage and voodoo band compression to reduce swelling and stiffness.Dry needling to relieve pain and improve muscle activation.24/7 compression sleeve use to manage swelling and promote recovery.
Mid Phase: Rebuild Strength and Control
Once swelling subsides and motion returns, we shift focus toward building ankle strength, balance, and coordination.
This stage bridges basic movement and athletic function — restoring your ankle’s ability to stabilize under everyday and athletic demands.Our focus:Progress range of motion and resistance training.Introduce balance and proprioception drills on stable and unstable surfaces.Continue managing any residual swelling to ensure smooth progress.
End Stage: Return to Power and Performance
The final stage is where athletes regain their explosiveness, agility, and sport-specific readiness.
We integrate plyometrics, cutting, and directional drills that mimic your sport’s real-world challenges — basketball jumps, soccer pivots, football sprints, and more.The goal: Build a resilient ankle capable of handling rapid movements, unpredictable landings, and high-impact demands — without fear or instability.Ready to Start Your Recovery?
Don’t let an ankle sprain keep you on the sidelines longer than it should. Whether you rolled your ankle last week or have been dealing with chronic instability for years, the right physical therapy approach can make all the difference.Schedule your ankle recovery evaluation today and take the first step toward getting back to the sport you love — stronger than before.Building Better Athletes: A Smarter Path Back to Sport
At J Sports Rehabilitation (JSR), we believe every injury is an opportunity to rebuild and come back stronger. Our mission is to bridge the gap between injury rehabilitation and full return to sport or activity through a collaborative, athlete-centered approach….
At J Sports Rehabilitation (JSR), we believe that every setback is an opportunity for growth. When an athlete is injured, it’s not just about recovery — it’s a chance to rebuild, re-establish proper movement patterns, and strengthen the body as a whole. Injury can be the beginning of a smarter, stronger return to sport.
When professional athletes get hurt, they’re supported by a full team — doctors, physical therapists, athletic trainers, and performance coaches — all working together to create the best possible outcome. At JSR, we believe this level of coordinated care shouldn’t be reserved for elite athletes.
Our mission is to bridge the gap between injury rehabilitation and full return to sport or daily activity. You don’t need to play professionally to deserve a team dedicated to your recovery — and your success.Comprehensive Sports Rehabilitation for Every Athlete
We work with adults and young athletes recovering from knee, hip, foot/ankle, shoulder, and back surgeries. Our goal is to collaborate seamlessly with your medical providers and strength and conditioning coaches to ensure a smooth, safe, and effective recovery.
Whether you’re returning from an ACL reconstruction, rotator cuff repair, hip labral surgery, or a muscle strain, our team helps you progress confidently back to the sport or activity you love. Every plan is customized to your goals — from rebuilding strength and stability to restoring speed, power, and confidence in movement.The Return to Sport Difference
Our Return to Sport Program was designed to give every athlete access to the same high-quality, team-based care used at the professional level.In the early phases of recovery, your physical therapist leads the process, focusing on healing, mobility, and proper movement patterns. As you advance, we begin to integrate modified strength training with your coach to prepare you for full performance.For example:If you’re recovering from an ACL injury, your strength coach can guide upper-body development during the early recovery phase.If you’re rehabbing a shoulder injury, your coach can focus on lower-body strength to maintain balance and progress.
This collaborative model ensures your entire body continues to improve — not just the injured area.A Team Approach to Athletic Recovery
At JSR, our team communicates across disciplines — sharing updates, insights, and progress notes to make sure your rehabilitation, strength training, and performance goals align perfectly. The result is a seamless transition from rehab to training to competition.The goal is simple: to help you return stronger, more balanced, and more resilient than before.In partnership with SPECTRUM Performance and Competitor Performance Academy, we don’t just help you recover — we help you build a better athlete.